Suprane (desflurane)
The fast-acting anesthetic agent with low solubility1,2 in blood and tissues designed to help facilitate precise intraoperative control and rapid recovery.3,4

Having the lowest solubility of all anesthetic gases, Suprane (desflurane) offers fast wash-in and wash-out, swift control during surgery, and a rapid recovery for your patients.1,5 These features effectively make Suprane suitable for a wide range of patients and procedures, and particularly useful for patients in need of a fast recovery and earlier discharge from the hospital.

Meeting unique patient needs is critical for anesthesia recovery
We know that all patients are not the same. Changes in medical practice around surgeries mean that anesthesiologists need options for the optimal drug for each unique patient.
With populations of elderly patients growing, the predominance of obese patients increasing, the move to efficient same-day and ambulatory surgeries, and the implementation of ERAS protocols – anesthesiologists need a wide variety of options for induction, maintenance, and recovery from anesthesia.1,5
Video testimonials
Video testimonials
Video testimonials

Anesthetic agents with low solubility play an important role in recovery
In at-risk patient groups, like elderly and obese patients, as well as for procedures like neurosurgery, pulmonary surgery and cholecystectomy, precise intraoperative control and rapid recovery is desired. This can be achieved by using fast-acting anesthetic agents with a low solubility in blood and tissues.1, 6-10

Suprane’s low solubility results in precise control and fast, early recovery
Suprane has low blood and tissue solubilities. Its blood: gas partition coefficient is like that of nitrous oxide, and lower than that of sevoflurane and especially isoflurane. Suprane’s solubility in tissue is lower than for all the current halogenated inhaled anesthetic agents.1,11,19
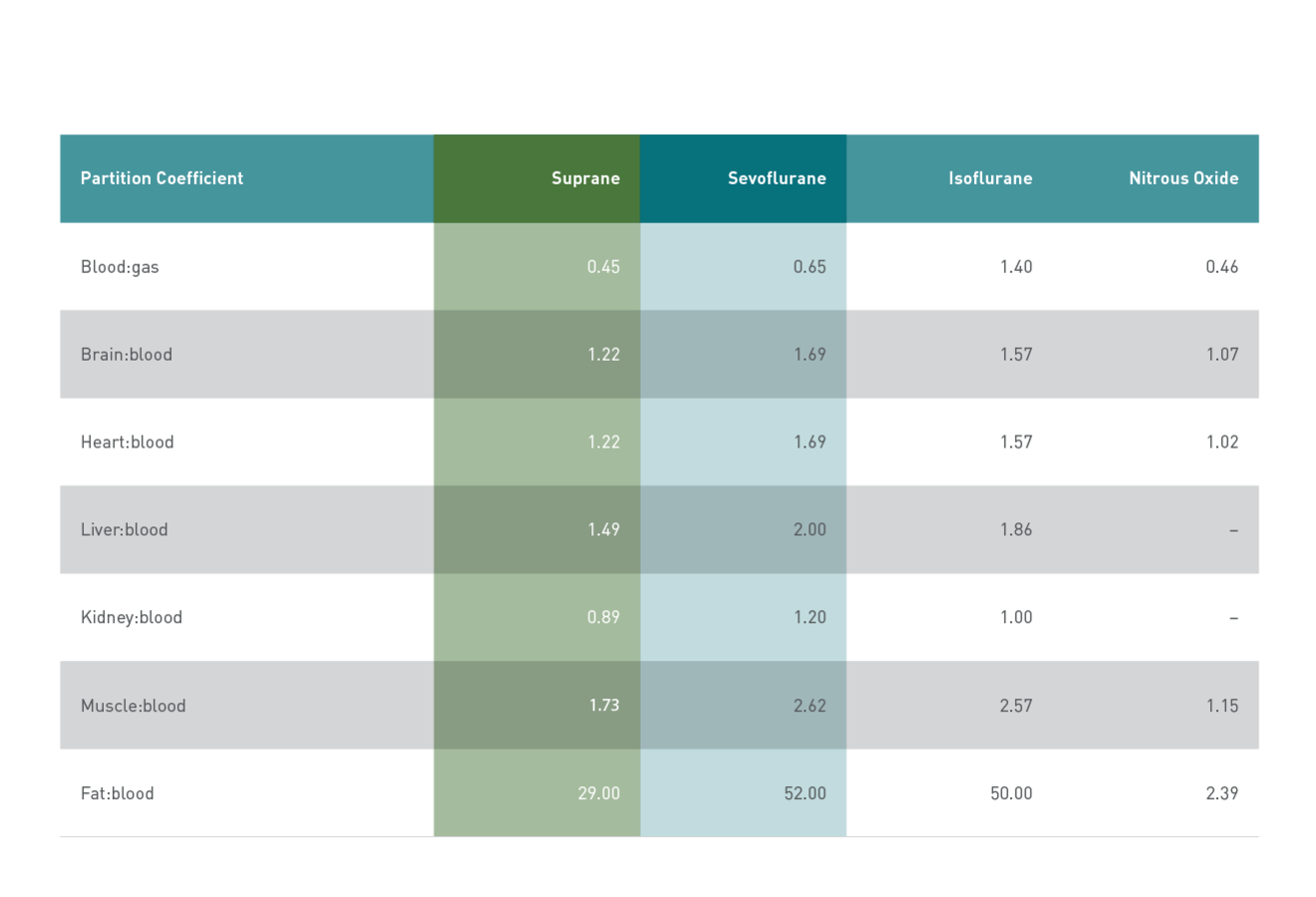
Partition coefficients of potent inhaled anesthetic agents
These favorable kinetic properties drive Suprane’s fast onset and offset and make it useful for precise control over acute, intraoperative changes in blood pressure and heart rate.5
After surgery, Suprane’s low solubility helps ensure an early and predictable recovery, making Suprane an optimal choice for post-anesthesia care. Rapid emergence and favorable recovery have been demonstrated across a wide range of patients and surgical interventions.7, 12-17

In a study of maintenance anaesthesia in 60 patients undergoing short day-case gynaecological surgery12
Faster full ambulant recovery
In a study of maintenance anaesthesia in 60 patients undergoing short day-case gynaecological surgery, 90% of day-case patients receiving Suprane returned to full ambulant activity the day following surgery, compared with 52% of patients receiving sevoflurane (p<0.01).12
Faster recovery without compromises
No difference was reported between Suprane and svoflurane groups in sleep disturbance, discomfort, analgesic consumption, or appetite.12

Faster wash-in and wash-out
Suprane has half the solubility of sevoflurane and the fastest wash-in and wash-out of all current potent halogenated inhaled anaesthetic agents.1-3
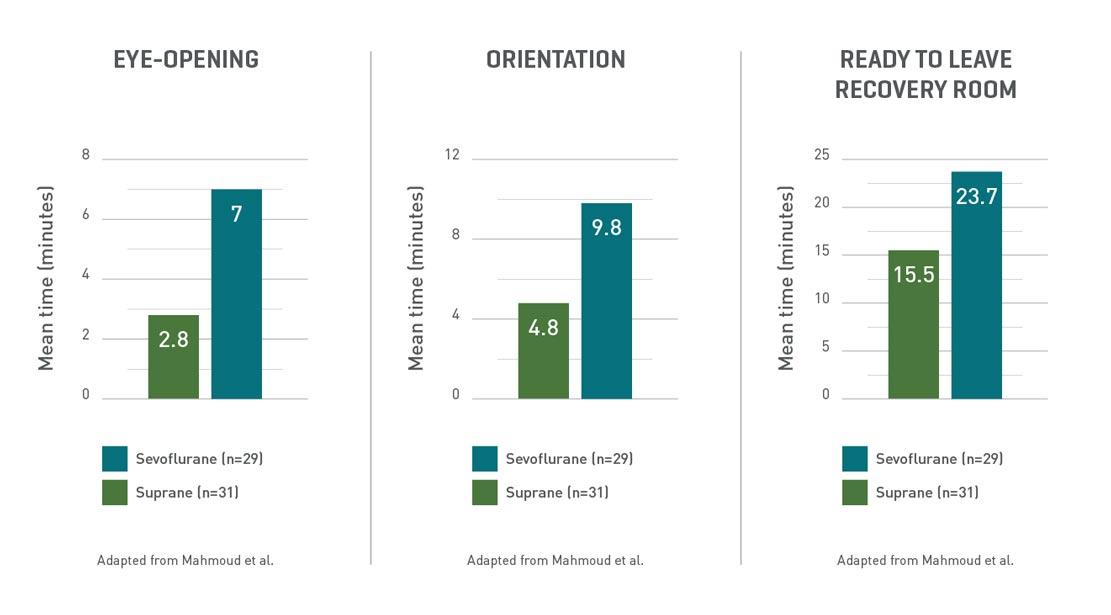
Suited for next day recovery
Suprane may offer rapid recovery in the surgical suite in day-case surgery. All assessments of early recovery were significantly faster in the Suprane (desflurane) group, compared with sevoflurane (p<0.0001).12*
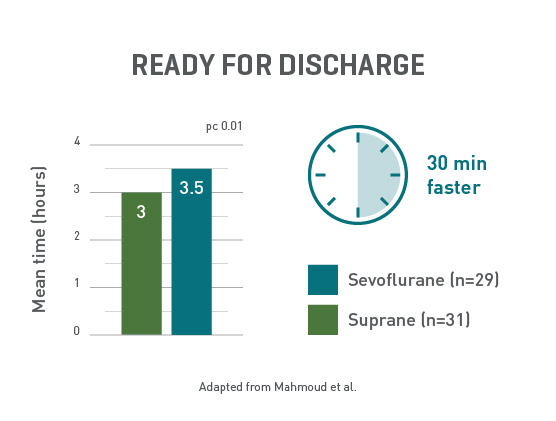
Ready to go home, faster
Day-case surgery patients receiving Suprane were ready for discharge at least 30 minutes faster than the sevoflurane group.12
*Maintenance anaesthesia with Suprane was initially 2−6%, and sevoflurane was initially 0.5−2.0% in oxygen/nitrous oxide in 60 gynaecological day-case patients aged 16−75 years (ASA I−II). The gases were given by laryngeal mask airway, with the vapour concentrations adjusted to meet the surgical requirements. Induction was with intravenous metoclopramide, fentanyl, and propofol. Mean duration of maintenance anaesthesia was 18 minutes in each group. Mean end-tidal vapour pressure at 5 and 10 minutes after induction was 4.5% for Suprane and 1.7% for sevoflurane, indicating that approximately equipotent concentrations of the two agents were given. Blood pressure and pulse rate at these times were similar in both groups.12